
 Zona McGee was blessed with a vibrant and beautiful little boy on July 2nd, 1993. She named him Ryan Andrew and fell in love with his sweet face the second she first held him. He looked just like her! Her husband, Kevin, and daughter Crystal, eight-years old at the time, were over the moon as well.
Zona McGee was blessed with a vibrant and beautiful little boy on July 2nd, 1993. She named him Ryan Andrew and fell in love with his sweet face the second she first held him. He looked just like her! Her husband, Kevin, and daughter Crystal, eight-years old at the time, were over the moon as well.
Zona had been battling a genetic kidney disorder her entire life, causing both of her pregnancies to be considered high-risk, so when her second delivery and birth went well, she was elated. She counted her blessings and relaxed into the day-to-day tasks of being a young mother. Her life was happy, and she adored her children very much.
By her beaming account, Ryan was a gregarious and charming little boy. “If there was something to explore, he would be all in it,” she told me. He had more energy than she knew what to do with and she kept him busy with stimulating activities and adventures. He was sweet, kind, and loved to make people smile, especially his sister, with whom he shared a unique bond.
Watching her children grow into responsible young adults made Zona immensely proud. She had many wonderful memories of her family through the years. Because her kidney disease is genetic, and other family members suffered as well, she had worried that her children may inherit the gene, but neither did. Ryan was a very bright, energetic, healthy child. Throughout his childhood, Ryan’s well-child checkups always received A+ reports.
However, when he was 15, his physician noted an incidental finding of minor scoliosis. Because Ryan did not complain of pain, the doctor decided to just keep an eye out for future changes. Ryan’s teenage years were happy. As he matured, his high energy settled down, and he became more introspective. He often spent his free time gaming on the computer, broadcasting on his YouTube channel, playing guitar, and enjoying life with his friends and family. Music was a major part of his world. He loved everything about it: listening, writing, and playing. He often shared his songs and favorite bands with his proud family.
 Ryan was a good student and took a local job after graduating from high school. He loved working and earning his own money. By all accounts, Ryan was a completely normal, functioning, and on-target, young adult. He was doing what most recent high school grads do – living life, having fun, and trying to decide what profession he might go into.
Ryan was a good student and took a local job after graduating from high school. He loved working and earning his own money. By all accounts, Ryan was a completely normal, functioning, and on-target, young adult. He was doing what most recent high school grads do – living life, having fun, and trying to decide what profession he might go into.
He was also heavily involved in organ donor awareness. Although Zona had been doing remarkably well for years, during this time, her condition began to rapidly decline, and she was put on a kidney donor list. She had a calling to act and started a blog, which led to a passionate fight to spread awareness about the importance of donating organs and tissue. Ryan fought alongside her and made the decision to become a donor himself. Little did they know, Ryan’s decision would end up saving many precious lives, including his own mother’s.
In May of 2013, Ryan began experiencing minor, intermittent headaches that were uncomfortable, but not debilitating. Zona made the logical assumption that Ryan was not wearing his glasses often enough. She continued to encourage him to wear his glasses, but the headaches became more severe over the next month. He visited his doctor who also believed it was due to his eyes, and advised Ryan to take Tylenol for the “migraines.” Stress was also considered, but the doctor was not a bit concerned.
Sadly, glasses and Tylenol did nothing to prevent or relieve the pain. His headaches were constant and progressively painful, making it difficult for Ryan to function. He was in agony, but he tried to minimize his suffering as to not “burden or stress out his family.” The doctors assured them that “nothing serious” was going on with him. The doctors were horribly premature in that assessment of Ryan’s symptoms.
One Friday, during a particularly bad flare up, Zona became very concerned that Ryan may have been suffering from a sinus infection and planned to take him to a walk-in clinic that following Monday. He never made it to that visit. On Sunday, May 12, 2013, Mother’s Day, Ryan was stricken, out of the blue, with an unbearable headache. He also complained of a stiff neck and collapsed in the bathroom. Zona and Crystal, who both heard a “thud” found Ryan unresponsive on the floor, and rushed him to the hospital.
They waited anxiously, for tests to come back, wondering if Ryan’s symptoms pointed to meningitis. The doctors mentioned that he, “May have a brain tumor”, before all the results were back. The family was terrified. However, after an MRI scan and lab results were completed, the doctor came in and told Ryan that “luckily” it was not a tumor or bacterial brain infection, but that they had found a Chiari Malformation.
Zona anxiously queried, “A what?”
Her question was ignored, as her child was an adult. She asked again, but the doctor turned from her and explained the test results to Ryan directly. He told Ryan that a Chiari occurs when the brainstem becomes herniated, but they could easily “fix” it with brain decompression surgery. He also told him that unless he agreed to surgery, his headaches would worsen, and he would just keep coming back to the E.R. He was presented with consent forms and was informed that they wanted to do the surgery the following morning.
Ryan had never dealt with illness or pain and he was terrified. After consulting with Zona, who felt that they should take some time to get more information, Ryan made the decision to undergo the operation. He just couldn’t bear the pain any longer; it was that debilitating. They were promising him relief and his symptoms were so severe, he trusted them and signed the consent forms. Zona was beside herself with worry. She thought to herself, “We just found out that he has something I have never even heard of, and they want to saw through his skull? I need more time!”
But she didn’t have time. She also did not have the respect of the doctor simply based on Ryan’s age. This infuriated her, as while Ryan was over 18, she felt that his family should be able to have their questions answered as well. But she didn’t fuss. They were coming to prep him, so she hid her fear and frustration to be strong for her son. When they wheeled the gurney away, she had no idea she would never see her son the same way again.
During Ryan’s first surgery, a temporary shunt was placed in an attempt to drain excess cerebrospinal fluid. When that failed, the surgeon made the call to do decompression surgery. Ryan went into this operation a very healthy and fit young man, but he came out with obvious signs of brain damage. Though it was clear that Ryan wasn’t well post-op, his family never again saw the surgeon who performed his decompression. There was no follow-up.
 Over the next few months, Ryan was rushed to the E.R. on several occasions due to cyclic, intractable, vomiting along with severe head and neck pain. During these dozen-plus visits to the E.R., he was turned away multiple times and labeled “drug-seeking, weak, and dramatic.” This was a slap in the face, as Ryan was advised to blindly have the surgery to prevent him from returning to the E.R. This painful irony was not lost on Zona, and it only added to her trauma and confusion.
Over the next few months, Ryan was rushed to the E.R. on several occasions due to cyclic, intractable, vomiting along with severe head and neck pain. During these dozen-plus visits to the E.R., he was turned away multiple times and labeled “drug-seeking, weak, and dramatic.” This was a slap in the face, as Ryan was advised to blindly have the surgery to prevent him from returning to the E.R. This painful irony was not lost on Zona, and it only added to her trauma and confusion.
Ryan was having seizures, yet he was told he was faking them. When Zona protested, she was told by a nurse entrusted with Ryan’s care, “Your son is not having seizures. What is wrong with you? Do you want him to have seizures?”
In all the E.R. visits, there was ONE brain scan. The family was told the surgery was successful and whatever was going on, if anything, was completely unrelated to his decompression surgery at their hospital.
 On the last visit to this particular hospital, the chief neurosurgeon refused to treat him neurologically and ordered a psychiatric evaluation instead. After speaking with Ryan, the psychiatrist said, “I do not believe you are crazy, but you are a bit of a wimp.”
On the last visit to this particular hospital, the chief neurosurgeon refused to treat him neurologically and ordered a psychiatric evaluation instead. After speaking with Ryan, the psychiatrist said, “I do not believe you are crazy, but you are a bit of a wimp.”
Zona was livid and chased everyone out of his room. She then immediately took Ryan to another, smaller hospital. It was obvious to the triage nurse that Ryan was in serious trouble. He was gaunt, having lost 30-plus pounds in three months. He had nystagmus, and his vital signs reflected the pain and distress he was experiencing. Scans showed brainstem slumping and his neck, literally, had no support. Zona was told that “too much bone had been removed,” and that he needed emergent intervention.
The doctors recommended immediate surgery to correct the horribly botched decompression. However, they suspected that he had meningitis, due to a fever, so they wanted to confirm and aggressively treat that before opening him back up. They began I.V. antibiotics and Dilaudid.
Again, Zona helplessly waited by his side for more test results. She was slightly relieved that there was finally a team of people looking after her child who believed them, but as she watched her child dozing from the pain medication, she barely recognized him. He was thin, with hollow, sunken eyes, and his weak, frail arms were drawn to his chest. Hands clenched in fists, he laid in a semi-fetal position. She wanted to know how this had happened. It had been a surreal, awful three months, and she wondered if there would be enough time to save him. Tragically, there was not.
Ryan suffered a fatal seizure the following morning that collapsed his brainstem, and he never woke up. He was pronounced brain dead, August 11th, 2013.
After Ryan’s death, it was discovered that he did not have an infection at all. According to an independent attorney’s assessment of Ryan’s medical records, there were at least nine opportunities for the health professionals, whom Zona trusted, to save Ryan’s life. The investigator called Ryan’s treatment barbaric and inconceivable. He, like all of us, want to know how this young man was so callously discarded and left to suffer until his untimely death. That question will never be answered. It is incomprehensible how the “professionals” who did have contact with Ryan, not only shunned him, but covered up evidence of medical injustice in order to protect their establishments, surgeons, and other health care workers.
Ryan’s severe, post-decompression, decline was obvious. Ryan was aware that he was in critical condition. He knew he was not going to survive. Before he died, he told Zona, “Make sure everyone knows what happened.” She did that and more.
Zona wanted the world to know who Ryan was and about the loving gifts he left behind. The medical establishment failed Ryan and his family, but he remains a true hero. Upon his death, several families received the gift of life through Ryan’s organ donation-including his mother, Zona. The day after Ryan died, she was in surgery receiving her child’s kidney.
There are times when Zona, naturally, wondered what she could have done differently, but the answer to that is simple: Without advocacy and awareness, hindsight is 20/20. There was nothing more she could have done. She tried everything in her power that she knew to do at that time. Because this was being reiterated by the doctors, she had faith that he was in good hands and that he would recover fully. There was no playbook she could consult on how to advocate for her child. She was in a surreal state of shock, disbelief and fear. She had no frame of reference to show her that the medical professionals in charge of Ryan’s care were terribly wrong, and negligent in the very least. She had to believe the doctors whose opinions and advice we are taught to trust. After all, doctors are the ones who have the medical degrees and they know best, right? No.
From the time Ryan was decompressed to the day he died, Zona made several calls to get Ryan help, but nobody would listen! Zona’s desperate attempts to alert the medical staff of Ryan’s worsening condition were to no avail. Nobody helped! Nobody cared! Nobody listened.
Zona took the pain from this unimaginable nightmare and turned into an unrelenting drive to educate other families who are caught up in the trap of medical injustice. She became a fierce advocate for patient safety and rights with the hope that no other child will suffer the way Ryan did. She also helped parents navigate the medical system so that they may learn from her experience. She vowed to work feverishly to bring about awareness and authorized a documentary about Ryan’s life and struggle with Chiari Malformation.
On Sunday, May 14th, 2017, Mother’s Day, Zona McGee, succumbed to metastatic lung cancer that she acquired from the anti-rejection drugs she was given to save Ryan’s kidney. Her death is a tremendous loss to our community. Her family and friends miss her more than any of my words can express.
Zona’s worst fear was that Ryan would be forgotten and that her promise, to let everyone know his story, would end with her life. I promised we will never let that happen. We never will.
Rest in peace, beautiful angels.
Please support Zona’s Visions:
Zona’s Blog Zona-Life On The Waitlist
Ryan’s Awareness Page: Ryan’s Voice Chiari Patient Awareness
Please support the documentary Writing For Ryan and view the documentary trailers and share the website link as well.
www.chiaridocumentary.com
Gianna Soares
Writing For Ryan
Updated 01-21-2018
For the exclusive use of Chiari Bridges, as per Zona’s request.
 MAINTAIN A POSITIVE ATTITUDE:
MAINTAIN A POSITIVE ATTITUDE: CHOOSING FOODS WITH YOU IN MIND:
CHOOSING FOODS WITH YOU IN MIND: MOVING IS ESSENTIAL TO MOBILITY:
MOVING IS ESSENTIAL TO MOBILITY:


 Chronic pain is something Chiarians face on a daily basis. Disabling pain that reduces your quality of life can make once simple tasks difficult to accomplish. Things like taking a shower or cooking become incredibly challenging. Fatigue can set in quickly, that even when we have plans that we’re excited about, just getting ready for them can be enough to put us back in bed. All of this can give us an altered self-perception of feeling useless, which enhances the depression. Chronic pain is both a physical and psychological condition, thus making treatment complex and difficult. Pain can cause depression and depression causes pain; it’s a vicious cycle.
Chronic pain is something Chiarians face on a daily basis. Disabling pain that reduces your quality of life can make once simple tasks difficult to accomplish. Things like taking a shower or cooking become incredibly challenging. Fatigue can set in quickly, that even when we have plans that we’re excited about, just getting ready for them can be enough to put us back in bed. All of this can give us an altered self-perception of feeling useless, which enhances the depression. Chronic pain is both a physical and psychological condition, thus making treatment complex and difficult. Pain can cause depression and depression causes pain; it’s a vicious cycle. Adjusting to the new normal is always a challenge, not only for us, but the ones we love as well. The loss of our former selves and our careers is very hard. Maybe you were a full-time parent or provider, caring for your family and you find yourself the one being cared for by loved ones. You find yourself depending on family and friends to do for you things that you once did for yourself, making you feel like a burden on those you love most. You may experience a sense of helplessness when trying to get friends and family to understand what you are going through. There will be friends and family who cannot or will not try to understand. They will think you are lazy or seeking attention. We must mourn the loss of old selves, careers, sometimes family and friends, as others must mourn their loss of your former self, and learn to embrace the new you in your new normal.
Adjusting to the new normal is always a challenge, not only for us, but the ones we love as well. The loss of our former selves and our careers is very hard. Maybe you were a full-time parent or provider, caring for your family and you find yourself the one being cared for by loved ones. You find yourself depending on family and friends to do for you things that you once did for yourself, making you feel like a burden on those you love most. You may experience a sense of helplessness when trying to get friends and family to understand what you are going through. There will be friends and family who cannot or will not try to understand. They will think you are lazy or seeking attention. We must mourn the loss of old selves, careers, sometimes family and friends, as others must mourn their loss of your former self, and learn to embrace the new you in your new normal.



 churches), as well as state and federal programs. Just are few examples of help available are assistance with mortgage, rent, utilities, food, clothing, medical bills, medical insurance, free or reduced-cost prescriptions, holiday assistance, back-to-school, free or reduced-cost dental clinics, pro-bono legal help, cash assistance programs, etc.
churches), as well as state and federal programs. Just are few examples of help available are assistance with mortgage, rent, utilities, food, clothing, medical bills, medical insurance, free or reduced-cost prescriptions, holiday assistance, back-to-school, free or reduced-cost dental clinics, pro-bono legal help, cash assistance programs, etc.





 Pain from a Chiari headache can be brought on from the simplest of things – a sneeze, a cough, laughter, or bearing down when going to the bathroom. We never know when the headache is going to strike, how long it will last, or when it will end. We are unable to describe the intensity of the pain to others, and when asked to rate our pain on a scale of 1 – 10, we want to scream, “14!” The radiating, crushing pain of the headaches robs us of our ability to function for days on end. And depending on the extent of damage the Chiari has caused you may also have the burning, stabbing, and shooting involved with neuropathic pain and neuralgia. The frosting on the pain cake, perhaps? With the many co-morbid disorders that go hand in hand with Chiari, such as Ehlers-Danlos Syndrome, Intracranial Hypertension, Hydrocephalus, and Tethered Cord Syndrome, is it any wonder we cry out, “Make it stop!”?
Pain from a Chiari headache can be brought on from the simplest of things – a sneeze, a cough, laughter, or bearing down when going to the bathroom. We never know when the headache is going to strike, how long it will last, or when it will end. We are unable to describe the intensity of the pain to others, and when asked to rate our pain on a scale of 1 – 10, we want to scream, “14!” The radiating, crushing pain of the headaches robs us of our ability to function for days on end. And depending on the extent of damage the Chiari has caused you may also have the burning, stabbing, and shooting involved with neuropathic pain and neuralgia. The frosting on the pain cake, perhaps? With the many co-morbid disorders that go hand in hand with Chiari, such as Ehlers-Danlos Syndrome, Intracranial Hypertension, Hydrocephalus, and Tethered Cord Syndrome, is it any wonder we cry out, “Make it stop!”? By a wide margin, the hardest part of our fight is dealing with doctors. One would think it would be the never-ending pain, but when your doctors do not believe you, ridicule you, or outright verbally abuse you, it not only adds insult to injury, but it probably illustrates reasons that your doctor(s) just might be the ones that need counseling. As patients, we are paying for them to help us with our medical problems; what we get instead is usually a referral to a therapist because of their ineptitude. The absurd part of this circle of insanity is that when we make ourselves more knowledgeable about our condition(s), because we have no other choice, a doctor that understand the Hippocratic Oath would respond by making themselves more knowledgeable as well, so they can help their patients. Yet, what is far too common are doctors that do not want to know the results of studies, who are complacent with their fifteen minutes of Chiari education, and think if they talk a good game, patients can be manipulated into thinking maybe it’s all in their minds.
By a wide margin, the hardest part of our fight is dealing with doctors. One would think it would be the never-ending pain, but when your doctors do not believe you, ridicule you, or outright verbally abuse you, it not only adds insult to injury, but it probably illustrates reasons that your doctor(s) just might be the ones that need counseling. As patients, we are paying for them to help us with our medical problems; what we get instead is usually a referral to a therapist because of their ineptitude. The absurd part of this circle of insanity is that when we make ourselves more knowledgeable about our condition(s), because we have no other choice, a doctor that understand the Hippocratic Oath would respond by making themselves more knowledgeable as well, so they can help their patients. Yet, what is far too common are doctors that do not want to know the results of studies, who are complacent with their fifteen minutes of Chiari education, and think if they talk a good game, patients can be manipulated into thinking maybe it’s all in their minds. In a distant second, would have to be the heart-wrenching feeling we get when our loved ones put more stock in the opinions of our morally bankrupt doctors, even once we have shared study after study and article after article showing you that our doctors are wrong. What we go through, feeling like our bodies have betrayed us, knowing that our doctors have betrayed us (even if it is because they do not know any better), we need you in our corner. This is the fight of our lives, for our lives, and we should never have to do it alone! The energetic, feisty, loving person that you have loved so much over the years is still inside of us! When your brain falls into your
In a distant second, would have to be the heart-wrenching feeling we get when our loved ones put more stock in the opinions of our morally bankrupt doctors, even once we have shared study after study and article after article showing you that our doctors are wrong. What we go through, feeling like our bodies have betrayed us, knowing that our doctors have betrayed us (even if it is because they do not know any better), we need you in our corner. This is the fight of our lives, for our lives, and we should never have to do it alone! The energetic, feisty, loving person that you have loved so much over the years is still inside of us! When your brain falls into your  (apparently, they do not know the importance of the Central Nervous System either). Although benefits can still be fought for and awarded, the fight becomes far more difficult than it needs to be. Chiarians often must fight for years, filing appeal after appeal, to prove that their reality is the reality.
(apparently, they do not know the importance of the Central Nervous System either). Although benefits can still be fought for and awarded, the fight becomes far more difficult than it needs to be. Chiarians often must fight for years, filing appeal after appeal, to prove that their reality is the reality.![The Christopher Ellington Story – A Chiari Warrior’s Journey [Updated]](https://dev.chiaribridges.org/wp-content/uploads/2017/05/hosp1.jpg)




 One of the biggest hurdles a Chiari patient may face is that of simply being diagnosed. Some studies cite an average of 5 years between the onset of symptoms significant enough for a patient to seek medical care and the patient receiving an accurate diagnosis of Chiari Malformation. Sadly, however, online support groups and message boards are peppered with the stories of patients who went undiagnosed, or more often, misdiagnosed, for decades. Patients are frequently misdiagnosed with conditions such as Fibromyalgia, Multiple Sclerosis, Chronic Fatigue Syndrome, Chronic Migraine, and various autoimmune disorders. Even more disturbing is the fact that in a study by Dr. Thomas Milhorat of over 300 patients diagnosed with Chiari, 59% had been diagnosed with a psychosomatic illness.
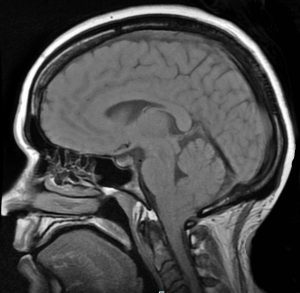
One of the biggest hurdles a Chiari patient may face is that of simply being diagnosed. Some studies cite an average of 5 years between the onset of symptoms significant enough for a patient to seek medical care and the patient receiving an accurate diagnosis of Chiari Malformation. Sadly, however, online support groups and message boards are peppered with the stories of patients who went undiagnosed, or more often, misdiagnosed, for decades. Patients are frequently misdiagnosed with conditions such as Fibromyalgia, Multiple Sclerosis, Chronic Fatigue Syndrome, Chronic Migraine, and various autoimmune disorders. Even more disturbing is the fact that in a study by Dr. Thomas Milhorat of over 300 patients diagnosed with Chiari, 59% had been diagnosed with a psychosomatic illness. Diagnosis of Chiari Malformation is based upon the presence of Chiari symptoms, such as an occipital headache that is brought about or worsened by Valsalva maneuvers, neurological symptoms such as poor balance, numbness or tingling in the arms, weakness in the legs, etc. combined with the “gold standard” of imaging studies for Chiari, an MRI of the brain.
Diagnosis of Chiari Malformation is based upon the presence of Chiari symptoms, such as an occipital headache that is brought about or worsened by Valsalva maneuvers, neurological symptoms such as poor balance, numbness or tingling in the arms, weakness in the legs, etc. combined with the “gold standard” of imaging studies for Chiari, an MRI of the brain. becoming apparent that Chiari is not quite as rare as it was once thought to be. When a primary care physician is stumped by a patient’s complaints of headaches and neurological symptoms, it is only natural to refer that patient to a neurologist for evaluation. But even many neurologists are grossly uninformed about Chiari. Many patients, even with an MRI that shows a herniation, are told that their many varied symptoms can’t possibly be due to the herniation of their brain, even with numerous studies available which show otherwise. Some patients have even been told by neurologists and even neurosurgeons that “Chiari doesn’t cause headaches [pain].” In fact, most symptomatic patients experience severe headaches, nerve pain, and pain from related disorders such as Syringomyelia.
becoming apparent that Chiari is not quite as rare as it was once thought to be. When a primary care physician is stumped by a patient’s complaints of headaches and neurological symptoms, it is only natural to refer that patient to a neurologist for evaluation. But even many neurologists are grossly uninformed about Chiari. Many patients, even with an MRI that shows a herniation, are told that their many varied symptoms can’t possibly be due to the herniation of their brain, even with numerous studies available which show otherwise. Some patients have even been told by neurologists and even neurosurgeons that “Chiari doesn’t cause headaches [pain].” In fact, most symptomatic patients experience severe headaches, nerve pain, and pain from related disorders such as Syringomyelia.