INTRACRANIAL HYPERTENSION (IH) AND IDIOPATHIC INTRACRANIAL HYPERTENSION (IIH) ARE CONNECTED, BUT ARE NOT THE SAME THING AND THEREFORE SHOULD NOT BE USED INTERCHANGEABLY.
 Intracranial Hypertension (IH) means high pressure inside the skull. Intracranial Pressure (ICP) is measured in millimeters of mercury (mmHg). Most scholars agree that on average, “normal pressure” should be between 5-15 mmHg and that 20-25 mmHg is when the ICP crosses the line into being IH. Pressure can be brought on by several different means: space-occupying masses such as hydrocephalus and cranial cysts/tumors; cranial edema (Encephalitis); trauma; stroke; aneurysm; certain infections/diseases (Meningitis), liver failure[1], kidney failure[2]; or as a side-effect of certain medications (such as: Tetracycline[3][5], Sulfasalazine[4], Lithium[5], excess amounts of Vitamin A, steroid use[6], growth hormone treatments[6], and the hormonal Intrauterine Device (IUD), “Mirena”[7]); however, sometimes the cause of the pressure is completely unknown. When an etiological cofactor exists, it is considered Secondary Intracranial Hypertension (SIH); when no other cause is identified, it is known as Idiopathic Intracranial Hypertension (IIH) or Primary Intracranial Hypertension (PIH).
Intracranial Hypertension (IH) means high pressure inside the skull. Intracranial Pressure (ICP) is measured in millimeters of mercury (mmHg). Most scholars agree that on average, “normal pressure” should be between 5-15 mmHg and that 20-25 mmHg is when the ICP crosses the line into being IH. Pressure can be brought on by several different means: space-occupying masses such as hydrocephalus and cranial cysts/tumors; cranial edema (Encephalitis); trauma; stroke; aneurysm; certain infections/diseases (Meningitis), liver failure[1], kidney failure[2]; or as a side-effect of certain medications (such as: Tetracycline[3][5], Sulfasalazine[4], Lithium[5], excess amounts of Vitamin A, steroid use[6], growth hormone treatments[6], and the hormonal Intrauterine Device (IUD), “Mirena”[7]); however, sometimes the cause of the pressure is completely unknown. When an etiological cofactor exists, it is considered Secondary Intracranial Hypertension (SIH); when no other cause is identified, it is known as Idiopathic Intracranial Hypertension (IIH) or Primary Intracranial Hypertension (PIH).
“Idiopathic Intracranial Hypertension (IIH) was first noticed in 1893, by the German physician Heinrich Quincke, who named it Serous Meningitis. As its absence of space occupying masses/lesions began to draw more thought, it was renamed Pseudotumor Cerebri (PTC) by Max Nonne in 1904. Sometime later, the term “Benign Intracranial Hypertension” began being used interchangeably with Pseudotumor Cerebri, to describe the fact that while it is sharing some of the same characteristics that a cranial tumor would cause, it is benign (not harmful), but arguments were made against it in that blindness is not indicative of being benign.”[6] The name finally settled as “Idiopathic Intracranial Hypertension,” which means IH of an unknown cause. No matter what you choose to call it, the pain and damage remains the same for those who have it.
UNDERSTANDING IDIOPATHIC INTRACRANIAL HYPERTENSION
IIH is a neurological disorder where the cerebrospinal fluid within the skull is elevated, without the presence of a space-occupying mass, edema (brought on by things such as trauma, infection, or disease), or any adverse reactions to certain medications. Studies show that IIH is more common amongst women between the ages of 20 and 50,[8] and there is a slight increase amongst those that are overweight. Some studies also suggest a connection between obstructive sleep apnea and transverse cerebral venous sinus stenosis.[9] Amongst the general population, IIH is believed to exist in 1/100,000 (0.00001). Amongst those that are 10% above their ideal body weight, the numbers increase to 13/100,000 (0.00013), and rising to 19/100,000 (0.00019) in those 20% above their ideal body weight.[10] Although doctors often tend to pass this off as merely a side effect of weight gain, the increase is slim and seems to decrease as the percentage of weight gain above ideal weight continues to rise above the 10% margin. 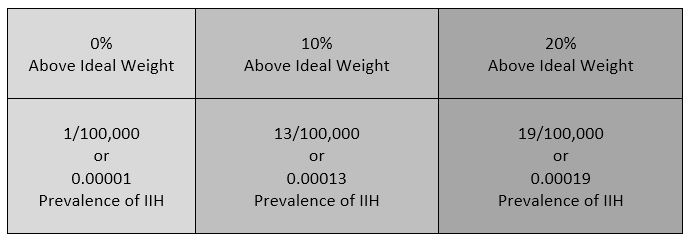 Additionally, the weight factor excludes men and children under the age of 10, which may simply be because women are more likely than men to have comorbid conditions that would lead to Intracranial Hypertension. Studies show that the women to men ratio for Chiari Malformation is believed to be 3:1 and those with both Chiari Malformation and Ehlers-Danlos Syndromes 9:1[11]). However weight is not irrelevant with IIH, the overweight/obese patient population report finding improvement of some symptoms when weight loss of 5-10% of one’s overall body weight, when accompanied by a low-salt diet[12].
Additionally, the weight factor excludes men and children under the age of 10, which may simply be because women are more likely than men to have comorbid conditions that would lead to Intracranial Hypertension. Studies show that the women to men ratio for Chiari Malformation is believed to be 3:1 and those with both Chiari Malformation and Ehlers-Danlos Syndromes 9:1[11]). However weight is not irrelevant with IIH, the overweight/obese patient population report finding improvement of some symptoms when weight loss of 5-10% of one’s overall body weight, when accompanied by a low-salt diet[12].
UNDERSTANDING THE IH/IIH CONNECTION: THE MONRO-KELLIE DOCTRINE
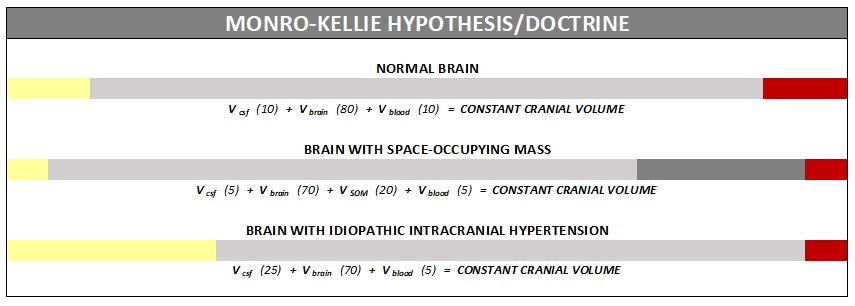
The association between IH/IIH and Chiari Malformation, appears to be a malicious intricate pathological circle. The cranium (skull) consists of brain matter, cerebrospinal fluid, and both venous and arterial blood. A hypothesis, referred to as the Monro-Kellie Hypothesis (or Monro-Kellie Doctrine), states, “The sum of volumes of brain, CSF, and intracranial blood is constant. An increase in one should cause a decrease in one or both of the remaining two.”[13] Therefore, if there is an abundance of cerebrospinal fluid (IIH or hydrocephalus), both cranial blood volume and brain matter should be forced to deplete. This depletion is usually directed in the path of least resistance – through the foramen magnum and into the spinal canal. When the cranial brain matter closest to the bottom of the skull (cerebellar tonsils) goes through the foramen magnum and into the spinal canal (an Acquired Chiari Malformation), it blocks the flow of cerebrospinal fluid, which in turn, continues to raise intracranial pressure.
SYMPTOMS OF INTRACRANIAL HYPERTENSION
Intracranial Hypertension (IH) can be either acute or chronic and comes with a variety of symptoms, many of which can help distinguish IH pain from typical pain associated with Chiari Malformation. A typical Chiari headache originates at the back of the skull (at the occiput), but IH headaches are usually described as pressure at the top of the head, that radiates downward. Headaches tend to be worse when laying down (which is opposite of low pressure headaches that are often relieved by laying down). Those that suffer from IH, often report waking up from sleep with a bad headache, and often a slight incline can help alleviate the headache pain. Pulsatile Tinnitus occurs when you hear a ringing in your ears that coincides with your heart beat. The tale-tell symptom of IH involves the damage done to the optical nerves. Papilledema is when the optic discs swell in response to the increased cranial pressure.[14] Symptoms of Papilledema include: headaches behind the eyes, blurred vision, fleeting vision, dimmed vision, double vision, visual obscurations, decreased peripheral vision, and photopsia. Another source of IH damage is seen in the pituitary gland and is known as Empty Sella Syndrome (ESS). As the high intracranial pressure (ICP) tries to take over, cerebrospinal fluid finds its way to the sella turcica and starts filling it with spinal fluid (partially or completely)[15]. The intruding CSF attempts to envelope this depression in the sphenoid bone, and squeezes the pituitary gland, flattening it until it appears “empty.” While some initially suffer no symptoms of the damage done to the pituitary gland, most eventually develop a variety of hormonal issues, known as hypopituitarism.
DIAGNOSIS CRITERIA
 Diagnosis of Intracranial Hypertension usually begins with investigating either the headaches or the vision problems. The least invasive test is having a neuro-ophthalmologist check behind your eyes for Papilledema. It is not considered conclusive in testing for IH, but it is essential in determining the extent of the damage to the optical nerves. Magnetic Resonance Imaging (MRI) of the brain can be useful in showing signs of Intracranial Hypertension. In cases where one or more space-occupying masses exists, further imaging and often biopsy may be required. The type of mass, its exact location, and the amount of damage that it is believed to be doing, will be used to determine the best treatment. If imaging gives an indication that the intracranial pressure is high, but no space-occupying mass exists, additional testing is usually necessary to confirm, some of which can be potentially be dangerous for those with Heritable Disorders of Connective Tissue (HDCT), such as Ehlers-Danlos Syndromes (EDS). Lumbar punctures (LP), also known as a spinal tap, are often used to test the
Diagnosis of Intracranial Hypertension usually begins with investigating either the headaches or the vision problems. The least invasive test is having a neuro-ophthalmologist check behind your eyes for Papilledema. It is not considered conclusive in testing for IH, but it is essential in determining the extent of the damage to the optical nerves. Magnetic Resonance Imaging (MRI) of the brain can be useful in showing signs of Intracranial Hypertension. In cases where one or more space-occupying masses exists, further imaging and often biopsy may be required. The type of mass, its exact location, and the amount of damage that it is believed to be doing, will be used to determine the best treatment. If imaging gives an indication that the intracranial pressure is high, but no space-occupying mass exists, additional testing is usually necessary to confirm, some of which can be potentially be dangerous for those with Heritable Disorders of Connective Tissue (HDCT), such as Ehlers-Danlos Syndromes (EDS). Lumbar punctures (LP), also known as a spinal tap, are often used to test the  opening CSF pressure, but by puncturing the dura (which is thinner than normal with Connective Tissue Disorders), the risk of a CSF leak is high. When an LP causes a CSF leak, the first indication is usually a post-dural-puncture headache (PLPH) and eventually, the intracranial hypertension will decrease, as the leak causes intracranial hypotension.[16] CSF leaks can escalate very quickly and can be difficult to identify and treat; therefore, we recommend that LPs be done only when absolutely necessary, and that they be done only under fluoroscopy, by qualified surgeons that fully understand the likelihood of Connective Tissue Disorders, the symptoms of leaks, and have a plan of action should those symptoms occur. Sometimes, ICP can fluctuate and have high spikes that cause problems, rendering LPs useless unless they are done at the precise time. When these spikes are suspected ICP monitoring bolts might be the better option, but still poses a risk of leaks.[17]
opening CSF pressure, but by puncturing the dura (which is thinner than normal with Connective Tissue Disorders), the risk of a CSF leak is high. When an LP causes a CSF leak, the first indication is usually a post-dural-puncture headache (PLPH) and eventually, the intracranial hypertension will decrease, as the leak causes intracranial hypotension.[16] CSF leaks can escalate very quickly and can be difficult to identify and treat; therefore, we recommend that LPs be done only when absolutely necessary, and that they be done only under fluoroscopy, by qualified surgeons that fully understand the likelihood of Connective Tissue Disorders, the symptoms of leaks, and have a plan of action should those symptoms occur. Sometimes, ICP can fluctuate and have high spikes that cause problems, rendering LPs useless unless they are done at the precise time. When these spikes are suspected ICP monitoring bolts might be the better option, but still poses a risk of leaks.[17]
TRANSVERSE SINUS STENOSIS (TSS)
Transverse sinus stenosis (TSS) occurs when there is a narrowing of the transverse sinus (dural venous sinus), which in turn can compromise cerebral venous outflow. TSS is common in idiopathic intracranial hypertension (IIH). Depending on the study that you are reading, it is proving to be present in 65-100% of those diagnosed specifically with IIH. Its direct connection seems relatively obscure, and there is no indication of its prevalence in intracranial hypertension (IH), but it is worth looking for and treating if found. While scholars remain undecided as to whether TSS is a cause or consequence of IH, if it does prove to be a cause of high pressure, IIH will likely no longer have an idiopathic element to it and it will become another etiology of Intracranial Hypertension. TSS can often be undetectable with standard Magnetic Resonance Imaging (MRI). The correct procedure would be Magnetic Resonance Venography (MRV, with the ATECO technique [18]), specifically looking for signs of stenosis, to include looking for fistula(s) and aneurysm(s). The lack of a fistula or aneurysms however, does not exclude the possibility of a TSS existing (remember it’s being found in 65-100% of those with IIH). Even with MRV, TSS can often be misinterpreted as “flow-related artifacts.” [18] Because the prevalence of TSS in IIH patients is high (some studies call it “universal”) [19], we recommend that all IIH patients have a MRV with the ATECO technique done before surgical treatment and that venous stenting be considered as a viable surgical treatment.
TREATMENT OPTIONS
Treatments for Idiopathic Intracranial Hypertension usually starts with weight loss and/or medicinal options; Diamox (Acetazolamide) and Topamax (Topiramate) are most frequently prescribed. Those with IH/IIH should avoid consuming caffeine, as it can increase pressure and therefore is counter-productive to treatment measures. Diamox is a carbonic anhydrase inhibitor and Topamax can also inhibit carbonic anhydrase, but is an anticonvulsant, often prescribed for the treatment of neuropathy and seizure disorders. Both are believed to successfully lower the production of cerebrospinal fluid. Topamax can also help suppress the appetite, which can help with weight loss, but it also comes with many side-effects like all nerve meds do. When medication fails to decrease ICP, a Ventriculoperitoneal Shunt (VP Shunt) or Ventriculoatrial Shunt (VA Shunt) are surgically placed to drain cerebrospinal fluid straight from the ventricle. Shunts are known for failing and often need a multitude of revisions. Venous stenting is not a new procedure, yet it is not readily offered. While there are studies indicating that the successful reduction of intracranial pressure can help with TSS. Stenting is not only a surgical treatment for the stenosis (which could significantly reduce the possibility of a life-threatening aneurysm in patients with a connective tissue disorder), but it is also a surgical treatment for intracranial hypertension as it “improves CSF resorption in the venous system.” [18] Therefore, it seems illogical to shunt (just dealing with the pressure) and leave such a potentially life-threatening condition untreated. [20] Studies are indicating as high as a 94% of patients being cured of all IIH symptoms as a direct result of venous stenting. [18] While all surgeries pose a risk of complications, and the statistics for stenting are likely inflated and skewed (like that of decompression surgeries), these statistics on stenting are definitely encouraging!
Intracranial Hypertension is a complex issue that should be explored whenever a Chiari Malformation exists, before a decompression surgery is performed. When both Intracranial Hypertension and Chiari Malformation are found to co-exist, the treatment should be in consideration of the correlation of the two, as they both are pathological co-factors of one another. Failure to recognize and treat Intracranial Hypertension before or soon after decompression surgery, will increase the likelihood of a failed decompression. While a decompression surgery can lower Intracranial Hypertension, as cerebrospinal fluid is once again allowed to flow, if space-occupying masses or a case of Idiopathic Intracranial Hypertension (where too much cerebrospinal fluid is being created) are left untreated, those problems will still exist after decompression surgery and the high pressure is likely to cause the cerebellar tonsils to fall once again.
*Revised October 2018
[wpedon id=”4396″ align=”center”]
References:
1 Jalan, R. “Intracranial Hypertension in Acute Liver Failure: Pathophysiological Basis of Rational Management.” Seminars in Liver Disease., U.S. National Library of Medicine, Aug. 2003, <www.ncbi.nlm.nih.gov/pubmed/14523680>.
2 Chang, D, et al. “Benign Intracranial Hypertension and Chronic Renal Failure.” Cleveland Clinic Journal of Medicine., U.S. National Library of Medicine, <www.ncbi.nlm.nih.gov/pubmed/1525975>.
3 Holst, Anders Vedel, et al. “A Severe Case of Tetracycline-Induced Intracranial Hypertension.”Dermatology Reports, PAGEPress Publications, 31 Jan. 2011, <www.ncbi.nlm.nih.gov/pmc/articles/PMC4211491/>.
4 Sevgi, E, et al. “Drug Induced Intracranial Hypertension Associated with Sulphasalazine Treatment.” Headache., U.S. National Library of Medicine, Feb. 2008, <www.ncbi.nlm.nih.gov/pubmed/18070060>.
5 Kelly, S J, et al. “Pseudotumor Cerebri Associated with Lithium Use in an 11-Year-Old Boy.”Journal of AAPOS : the Official Publication of the American Association for Pediatric Ophthalmology and Strabismus., U.S. National Library of Medicine, Apr. 2009, <www.ncbi.nlm.nih.gov/pubmed/19393521>.
6 Aylward, Shawn C. “Intracranial Hypertension: Is It Primary, Secondary, or Idiopathic?”Journal of Neurosciences in Rural Practice, Medknow Publications & Media Pvt Ltd, 2014, <www.ncbi.nlm.nih.gov/pmc/articles/PMC4173226/>.
7 Etminan, Mahyar, et al. “Risk of Intracranial Hypertension with Intrauterine Levonorgestrel.”Therapeutic Advances in Drug Safety, SAGE Publications, June 2015, <www.ncbi.nlm.nih.gov/pmc/articles/PMC4519742/>.
8 “Pseudotumor Cerebri Information Page.” National Institute of Neurological Disorders and Stroke, U.S. Department of Health and Human Services, <www.ninds.nih.gov/Disorders/All-Disorders/Pseudotumor-Cerebri-Information-Page>.
9 Thurtell, Matthew J., et al. “An Update on Idiopathic Intracranial Hypertension.” Reviews in Neurological Diseases, U.S. National Library of Medicine, 2010, <www.ncbi.nlm.nih.gov/pmc/articles/PMC3674489/>.
10 Wani, Irfan Yousuf, et al. “Complete Ophthalmoplegia: A Rare Presentation of Idiopathic Intracranial Hypertension.” Annals of Indian Academy of Neurology, Medknow Publications & Media Pvt Ltd, 2015, <www.ncbi.nlm.nih.gov/pmc/articles/PMC4683894/>.
11 Henderson, Fraser C., et al. “Neurological and Spinal Manifestations of the Ehlers–Danlos Syndromes.” American Journal of Medical Genetics Part C: Seminars in Medical Genetics, 21 Feb. 2017, <www.onlinelibrary.wiley.com/doi/10.1002/ajmg.c.31549/full>.
12 Thurtell, Matthew J., and Michael Wall. “Idiopathic Intracranial Hypertension (Pseudotumor Cerebri): Recognition, Treatment, and Ongoing Management.” Current Treatment Options in Neurology, U.S. National Library of Medicine, Feb. 2013,<www.ncbi.nlm.nih.gov/pmc/articles/PMC3554852/>.
13 Mokri, B. “The Monro-Kellie Hypothesis: Applications in CSF Volume Depletion.” Neurology., U.S. National Library of Medicine, 26 June 2001, <www.ncbi.nlm.nih.gov/pubmed/11425944>.
14 Schirmer, Clemens M, and Thomas R Hedges. “Mechanisms of Visual Loss in Papilledema.”Journal of Neurosurgery, <www.thejns.org/doi/full/10.3171/FOC-07/11/E5>.
15 “Empty Sella Syndrome Information Page.” National Institute of Neurological Disorders and Stroke, U.S. Department of Health and Human Services, <www.ninds.nih.gov/Disorders/All-Disorders/Empty-Sella-Syndrome-Information-Page>.
16 Panikkath, Ragesh, et al. “Intracranial Hypertension and Intracranial Hypotension Causing Headache in the Same Patient.” Proceedings (Baylor University. Medical Center), Baylor Health Care System, July 2014, <www.ncbi.nlm.nih.gov/pmc/articles/PMC4059569/>.
17 Abraham, Mary, and Vasudha Singhal. “Intracranial Pressure Monitoring.” Journal of Neuroanaesthesiology, <www.jnaccjournal.org/article.asp?issn=2348-0548;year=2015;volume=2;issue=3;spage=193;epage=203;aulast=Abraham>.
18 Ahmed, Wilkinson, et al. “Transverse Sinus Stenting for Idiopathic Intracranial Hypertension: A Review of 52 Patients and of Model Prediction.” American Society of Neuroradiology, July 2011. <www.ajnr.org/content/32/8/1408.long>.
19 Riggeal, Bruce, et al. “Clinical course of idiopathic intracranial hypertension with transverse sinus stenosis.” American Academy of Neurology, 2012. <www.ncbi.nlm.nih.gov/pmc/articles/PMC3589184/>.
20 Patel, et al. “Evaluating and treating venous outflow stenoses is necessary for the successful open surgical treatment of arteriovenous fistula aneurysms.” Society for Clinical Vascular Surgery, Volume 61, Issue 2. February 2015. <www.sciencedirect.com/science/article/pii/S0741521414014116>.

 Today is 11th April, 2019. Spring is in the air, yet I struggle to appreciate its presence. My daughters are at school, my son is at home in bed yet again. Like so many other days he is unable to get up. My son is 19 years old and looks just like any other 19 year old. You would never guess that this 19 year old is fighting a tremendously unfair battle every single day and has done so for several years.
Today is 11th April, 2019. Spring is in the air, yet I struggle to appreciate its presence. My daughters are at school, my son is at home in bed yet again. Like so many other days he is unable to get up. My son is 19 years old and looks just like any other 19 year old. You would never guess that this 19 year old is fighting a tremendously unfair battle every single day and has done so for several years. I started carrying out my own research, which clarified the distinct link between brain disorders and compromised immune/digestive systems. Whereas his doctors are reluctant to make that link, the evidence is clear. 18 months after surgery, my son got struck down by glandular fever. Again, we were hopeful that this would only be a temporary setback. Today however, my son suffers from chronic fatigue syndrome as well as dysautonomia.
I started carrying out my own research, which clarified the distinct link between brain disorders and compromised immune/digestive systems. Whereas his doctors are reluctant to make that link, the evidence is clear. 18 months after surgery, my son got struck down by glandular fever. Again, we were hopeful that this would only be a temporary setback. Today however, my son suffers from chronic fatigue syndrome as well as dysautonomia. My son is my hero. My son is a fighter. My son has generally done what health professionals told him to do, taken every medication health professionals told him to take, followed the advice health professionals told him to take, yet the system continues to let him down. When I look into my son’s eyes, I still see this steadfast determination but I now also see pain and disillusionment. My son believed me when I told him we would overcome this together. My son believed me when I told him the worst would be over soon. My son doesn’t believe me anymore. I feel that I have failed him.
My son is my hero. My son is a fighter. My son has generally done what health professionals told him to do, taken every medication health professionals told him to take, followed the advice health professionals told him to take, yet the system continues to let him down. When I look into my son’s eyes, I still see this steadfast determination but I now also see pain and disillusionment. My son believed me when I told him we would overcome this together. My son believed me when I told him the worst would be over soon. My son doesn’t believe me anymore. I feel that I have failed him.

 It leaves a hole in the hearts of the Chiari community because, even as dysfunctional as we are sometimes, we know we’re all in this together!
It leaves a hole in the hearts of the Chiari community because, even as dysfunctional as we are sometimes, we know we’re all in this together!  Her husband has had days where he was so petrified at the thought of losing her. Sometimes that fear manifested as anger and frustration, but it wasn’t her that he was really mad at; He was mad at the Chiari that was taking his wife from him. He regretted those words from the very minute that he gazed upon her eyes as she heard them. He couldn’t make her forget those words, they pierced her soul too deeply, so he internally committed to just try and show her why he loves her. Despite his frustrations with the situation, he admired this amazingly strong woman who was facing more pain than he could ever understand. He’s cried out to God privately for this soul mate that he committed to so many years ago. He feared losing her and he did not know how he could ever hold everything together like she did, but he had to try because there was so much was on his shoulders. He never talked much about the weight he carried in it all, because he knew what she was facing was already more than she could handle. So, he learned to grieve as silently as he could – to understand what he could, to empathize as he could, to remain as strong for her and the family as best as he could.
Her husband has had days where he was so petrified at the thought of losing her. Sometimes that fear manifested as anger and frustration, but it wasn’t her that he was really mad at; He was mad at the Chiari that was taking his wife from him. He regretted those words from the very minute that he gazed upon her eyes as she heard them. He couldn’t make her forget those words, they pierced her soul too deeply, so he internally committed to just try and show her why he loves her. Despite his frustrations with the situation, he admired this amazingly strong woman who was facing more pain than he could ever understand. He’s cried out to God privately for this soul mate that he committed to so many years ago. He feared losing her and he did not know how he could ever hold everything together like she did, but he had to try because there was so much was on his shoulders. He never talked much about the weight he carried in it all, because he knew what she was facing was already more than she could handle. So, he learned to grieve as silently as he could – to understand what he could, to empathize as he could, to remain as strong for her and the family as best as he could. Her children have learned to grieve in silence as well. They learned to face life and all the obstacles they faced without making waves at home. How could they? They saw the pain that flared when things had stressed her in the past. They didn’t want to cause that again. They longed having the mom that they used to have, the mom with the strength to climb every mountain with them, the mom that made every challenge in life seem conquerable. They admired her strength and never understood how they could admire so much in her yet hate the fact that she wasn’t always there for them anymore. Even when she so desperately tried to be there the brain fog often dominated and took over the conversation entirely, this conversation that she probably wouldn’t remember for long. They resented her for it but knew that it wasn’t her fault. Like everyone else that loved her the most, they said so many things that they regretted. They knew that they often came across like they hated her, but the real truth was there was no one in the world that they longed for more. They’ve always hated seeing her in pain, yet her pain served as a constant reminder of the future that they feared in their future. They remember when she told them about the hereditary nature of the genes passed on to them, with tears in her eyes. Would they have what she had? Would they become as symptomatic? Would they have the courage to fight it as valiantly as she did? Should they have children one day? The reasons for concern were endless.
Her children have learned to grieve in silence as well. They learned to face life and all the obstacles they faced without making waves at home. How could they? They saw the pain that flared when things had stressed her in the past. They didn’t want to cause that again. They longed having the mom that they used to have, the mom with the strength to climb every mountain with them, the mom that made every challenge in life seem conquerable. They admired her strength and never understood how they could admire so much in her yet hate the fact that she wasn’t always there for them anymore. Even when she so desperately tried to be there the brain fog often dominated and took over the conversation entirely, this conversation that she probably wouldn’t remember for long. They resented her for it but knew that it wasn’t her fault. Like everyone else that loved her the most, they said so many things that they regretted. They knew that they often came across like they hated her, but the real truth was there was no one in the world that they longed for more. They’ve always hated seeing her in pain, yet her pain served as a constant reminder of the future that they feared in their future. They remember when she told them about the hereditary nature of the genes passed on to them, with tears in her eyes. Would they have what she had? Would they become as symptomatic? Would they have the courage to fight it as valiantly as she did? Should they have children one day? The reasons for concern were endless. Depending on when she became symptomatic, her parents have likely spent endless days and nights in hospitals and emergency rooms. They’ve spent years learning all they could and even learned to recite her diagnoses with detailed explanations because they’d became so accustomed to these conditions that so few doctors could pronounce, much less treat. For years they made sure to always have her complete medical chart in hand with official documentation, in case they were challenged by a medical professional or anyone dared to call their daughter “a drug seeker” or “psychosomatic.” They spent countless hours trying to dull the tortuous pain they saw her go through, and spent many more hours researching creative home remedies to give her a sense of relief, even if it was only momentary. There were times they prayed for God to just go ahead and take her, so she wouldn’t be in anymore pain; and then felt guilty for even thinking it. Then one day the screaming stopped, the pain was gone, but with it so went their daughter.
Depending on when she became symptomatic, her parents have likely spent endless days and nights in hospitals and emergency rooms. They’ve spent years learning all they could and even learned to recite her diagnoses with detailed explanations because they’d became so accustomed to these conditions that so few doctors could pronounce, much less treat. For years they made sure to always have her complete medical chart in hand with official documentation, in case they were challenged by a medical professional or anyone dared to call their daughter “a drug seeker” or “psychosomatic.” They spent countless hours trying to dull the tortuous pain they saw her go through, and spent many more hours researching creative home remedies to give her a sense of relief, even if it was only momentary. There were times they prayed for God to just go ahead and take her, so she wouldn’t be in anymore pain; and then felt guilty for even thinking it. Then one day the screaming stopped, the pain was gone, but with it so went their daughter.
 Like any marriage, we’ve had our rocky moments. We’ve both showed our ugly sides more than we like to admit. I’m not sure when he changed, but somehow along the way in our 27 years of marriage, my husband morphed into this amazing man who is EXACTLY what I need in every way!
Like any marriage, we’ve had our rocky moments. We’ve both showed our ugly sides more than we like to admit. I’m not sure when he changed, but somehow along the way in our 27 years of marriage, my husband morphed into this amazing man who is EXACTLY what I need in every way! relieving all of my symptoms, but never in a million years did we think that decompression would open Pandora’s Box on my need for surgeries. From 2012-2015 I needed seven additional surgeries. Each surgery had its own recovery and complications. And with each additional surgery, I became increasingly dependent on my husband for help, but not once did he complain. This was affecting his life too, but not once did he concentrate on that. Not once did he think of it as being unfair to him to have to care for me, even though it really was. I’m now covered with scars on my left side from my neck to my groin, one night he raised my pajama shirt and gazed intensely upon them. He started kissing them. When he got to the scars covering my stomach, I pushed him away and with tears in my eyes, I told him that I wasn’t comfortable with him touching me there. He looked me in the eyes and told me that he didn’t see me the way that I see myself. He said that when he sees my scars, he’s reminded of all that I’ve had to fight through and what a strong woman he’s married to. “I wish that you could see yourself the way that I see you,” he exclaimed. All my insecurities just melted with his words of affirmation.
relieving all of my symptoms, but never in a million years did we think that decompression would open Pandora’s Box on my need for surgeries. From 2012-2015 I needed seven additional surgeries. Each surgery had its own recovery and complications. And with each additional surgery, I became increasingly dependent on my husband for help, but not once did he complain. This was affecting his life too, but not once did he concentrate on that. Not once did he think of it as being unfair to him to have to care for me, even though it really was. I’m now covered with scars on my left side from my neck to my groin, one night he raised my pajama shirt and gazed intensely upon them. He started kissing them. When he got to the scars covering my stomach, I pushed him away and with tears in my eyes, I told him that I wasn’t comfortable with him touching me there. He looked me in the eyes and told me that he didn’t see me the way that I see myself. He said that when he sees my scars, he’s reminded of all that I’ve had to fight through and what a strong woman he’s married to. “I wish that you could see yourself the way that I see you,” he exclaimed. All my insecurities just melted with his words of affirmation.

 I’m alive. I’m breathing. But I can’t touch any of the things that make me happy.
I’m alive. I’m breathing. But I can’t touch any of the things that make me happy.
 I’m in an abusive relationship. It’s not a romantic one at least, not in the traditional sense of the word.
I’m in an abusive relationship. It’s not a romantic one at least, not in the traditional sense of the word. Once I isolated myself from the people that I once would have laid my life down for, she turned it on me. There was no more self-love. Instead she instilled self-doubt. I wasn’t good enough to have friends and family, and love and happiness. I deserved her miserable and toxic company. All this emptiness was my fault and now I must live with it and her forever.
Once I isolated myself from the people that I once would have laid my life down for, she turned it on me. There was no more self-love. Instead she instilled self-doubt. I wasn’t good enough to have friends and family, and love and happiness. I deserved her miserable and toxic company. All this emptiness was my fault and now I must live with it and her forever. I started to hate her. I hated her for making me hate myself. And every time I would get close to telling her to stay away from me forever, I would get flashbacks of that goddess. The girl who laughed in the face of fear. The girl who made me feel the best I’ve ever felt. I know she’s still there. I can’t give up on her.
I started to hate her. I hated her for making me hate myself. And every time I would get close to telling her to stay away from me forever, I would get flashbacks of that goddess. The girl who laughed in the face of fear. The girl who made me feel the best I’ve ever felt. I know she’s still there. I can’t give up on her.![Brain Under Pressure – Understanding Intracranial Hypertension [Archived]](https://dev.chiaribridges.org/wp-content/uploads/2017/12/Fotolia_87985277_M.jpg)

 Palliative Care (pronounced “pal-lee-uh-tiv” care) is a subspecialty of medical care, where an interdisciplinary team of professionals (both medical and social) are committed to helping provide “relief from symptoms and stress” for patients with serious, life-altering illnesses, and their families.
Palliative Care (pronounced “pal-lee-uh-tiv” care) is a subspecialty of medical care, where an interdisciplinary team of professionals (both medical and social) are committed to helping provide “relief from symptoms and stress” for patients with serious, life-altering illnesses, and their families.  Misconceptions Surrounding Palliative Care:
Misconceptions Surrounding Palliative Care:  Primary Care Doctors (who are supposed to be offering referrals to Palliative Care for their patients with serious medical conditions) often fail to fully understand the spectrum of Palliative Care. Because of their faulty understanding, most of us are never offered Palliative Care, and when we request it, we are often told that it is equivalent to hospice care or set aside for hospice patients, and therefore they believe that we do not qualify. THEY ARE WRONG!
Primary Care Doctors (who are supposed to be offering referrals to Palliative Care for their patients with serious medical conditions) often fail to fully understand the spectrum of Palliative Care. Because of their faulty understanding, most of us are never offered Palliative Care, and when we request it, we are often told that it is equivalent to hospice care or set aside for hospice patients, and therefore they believe that we do not qualify. THEY ARE WRONG!


 When a person suffers from a chronic condition, we sometimes equate our value to how we feel. Chiari, Ehlers-Danlos, CSF Leaks, Chronic Fatigue Syndrome, etc. all cause pain. Sometimes we tend to carry that pain along with us as baggage. If we carry our self-value as related to pain, we are more likely to let healthcare professionals bully us and eventually, all this baggage compromises the relationships that matter most to us. Well, it’s time to look deep inside ourselves and find our inner strength.
When a person suffers from a chronic condition, we sometimes equate our value to how we feel. Chiari, Ehlers-Danlos, CSF Leaks, Chronic Fatigue Syndrome, etc. all cause pain. Sometimes we tend to carry that pain along with us as baggage. If we carry our self-value as related to pain, we are more likely to let healthcare professionals bully us and eventually, all this baggage compromises the relationships that matter most to us. Well, it’s time to look deep inside ourselves and find our inner strength. That’s right! YOU, with these chronic conditions, feeling as battered and bruised as you do, are like Superman or Superwoman. You have done more while enduring pain, than most people do that are completely healthy!
That’s right! YOU, with these chronic conditions, feeling as battered and bruised as you do, are like Superman or Superwoman. You have done more while enduring pain, than most people do that are completely healthy! When your doctor provides substandard care, he subjects himself/herself to a formal complaint. Misdiagnosis or delayed diagnosis that leads to incorrect treatment, delayed treatment, or no treatment at all, can cause you harm and is complaint worthy. Overprescribing, underprescribing, and failure to prescribe adequate treatment for your condition(s) are also grounds for a formal complaint.
When your doctor provides substandard care, he subjects himself/herself to a formal complaint. Misdiagnosis or delayed diagnosis that leads to incorrect treatment, delayed treatment, or no treatment at all, can cause you harm and is complaint worthy. Overprescribing, underprescribing, and failure to prescribe adequate treatment for your condition(s) are also grounds for a formal complaint.