
Craniocervical Instability and related pathologies of the craniocervical junction are an important topic for anyone diagnosed with Chiari 1 malformation. “Complex Chiari,” or the presence of craniovertebral abnormalities or instability in addition to the presence of cerebellar tonsillar herniation, is present in approximately one fourth of all cases of Chiari 1 malformation[1]. These cases usually involve the presence of a genetic connective tissue disorder and are thought by experts to be the cause of most Chiari decompression failures[2]. When the doctor and patient alike are not knowledgeable about these conditions and the additional symptoms that often accompany them, these more complex cases are often treated with a standard decompression, which can actually weaken the stability of the craniocervical junction more, and result in an increase of symptoms rather than a clinical improvement. Understanding what signs and symptoms to look for that may indicate that your Chiari is more complex, is vital in receiving the appropriate treatment the first time. This is especially important considering that, according to Chiari expert Paolo Bolognese, M.D., “[with revision surgeries], the results are not as good as if you had done the posterior decompression well the first time.”[3]
Punjabi and White define instability as the “loss of the ability of the spine under physiological loads to maintain relationships between vertebrae in such a way that there is no damage or subsequent irritation of the spinal cord, (brain stem) or nerve roots, and in addition that there is development of deformity or incapacitating pain due to structural changes.”[4] This means that the ligaments and muscles that normally hold the spine together, are too weak or damaged to handle the normal range of motion and weight of anatomic structures. For example, in Craniocervical Instability, the neck is not strong enough to support the normal weight of the head, without elements of the spine moving in such a way that it causes pain or damage to the nervous system (spinal cord, brain stem, and even cranial nerves). The result is that the bones that make up the lower skull and upper spine get pushed out of their normal anatomic location and begin to impinge on or cause stretching of these parts of the nervous system.
Craniocervical Instability can result from or be exacerbated by a trauma, such as a severe whiplash injury. However, many cases of CCI are associated with some sort of connective tissue disorder, such as a heritable disorder of connective tissue (HDCT, like Ehlers-Danlos Syndrome or Marfan’s), or an autoimmune condition that affects the connective tissue (such as Rheumatoid Arthritis), or a few other rarer conditions that affect the integrity of bony structures in the skull and spine. Instability can result either from lax ligaments and other connective tissues, soft bones (also seen in HDCTs) or from something like pannus formation, where repeated rubbing together of the joints causes a build-up of granulated tissue around bony structures and changes the way certain bones lie in relationship to one another[5]. Craniocervical Instability can also result as a complication of Chiari decompression surgery, when too much bone is removed from the skull, resulting in the instability of the skull on the top of the spine[6].
In the patient community, the term “CCI” is often used in reference to both Craniocervical Instability and Atlantoaxial Instability (AAI). CCI is often used to refer to the commonly seen combination of issues with the craniocervical junction, that include the instability of the joints where the skull meets the C1 vertebrae (which is true CCI), the instability of the joints between C1 and C2 (true AAI), a retroflexed odontoid, pannus formation, and a kyphotic clivo-axial angle (which are all forms of basilar impression/invagination). But CCI really should refer to the movement of the skull with respect to the spine. This sliding is referred to as “translation” and is measured on dynamic imaging in millimeters. The pathological threshold for the degree of translation of the basion with respect to the odontoid process between flexion and extension is 2mm, and any amount of translation greater than 1mm is capable of producing symptoms7. Likewise, at the C1-C2 joint, instability in the form of AAI can cause an excessive uncovering of the joint facets. Facets are the surfaces of the vertebrae that articulate with next vertebra. An uncovering of the facets that exceeds 20% is considered pathological.
The occipito-atlantic joint allows for about half of the cervical spine’s ability to flex and extend (tilt forward and backward). Likewise, the atlantoaxial joint [the articulation between C1 (atlas) and C2 (axis)] accounts for about half of the cervical spine’s ability to rotate the head. Because of this, these vertebrae lack the same amount of stability as the remainder of the spine, and ligaments are largely responsible for their stability[8]. Therefore, ligamentous laxity, as seen in connective tissue disorders, make these areas of the spine particularly prone to pathologic instability. Symptoms of AAI may include visual changes, syncope (fainting) or near-syncopal episodes, dizziness, nausea, facial pain, difficulty swallowing, choking, respiratory issues, and upper cervical tenderness. These symptoms will usually improve with the use of a neck brace[9]. For patients with connective tissue disorders, as are seen in 12-20% of patients diagnosed with Chiari, dynamic imaging is very important in identifying potential instability. The ideal tests to diagnose CCI and AAI are an upright MRI with flexion and extension and a 3D CT with rotational views, respectively[10]. It is important to note that ventral brain stem compression may not be seen on traditional supine MR imaging, while it may be very evident on dynamic imaging.
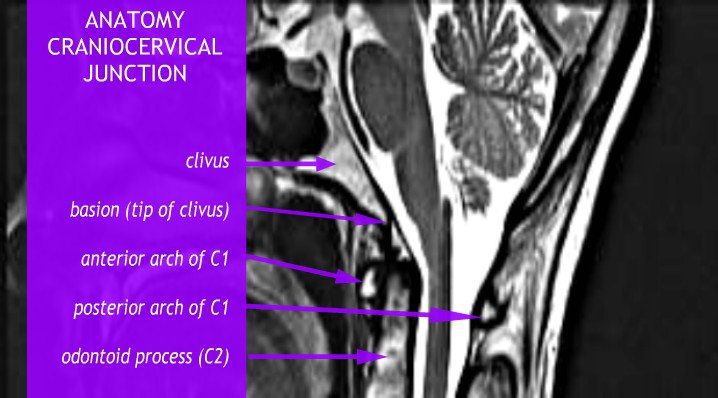
Basilar Invagination and Basilar Impression are also often seen with instability. They are almost identical to one another, and refer to upward displacement of the bones of the spine. However, technically, Basilar Invagination is caused by this deformation with normal bone, while Basilar Impression results from softening of bone[11]. For our purposes, this distinction is less important, but we will discuss any displacement in terms of “Basilar Invagination,” or “BI” for short. Forms of Basilar Invagination now include the prolapse of the odontoid process through the foramen magnum (the original condition described by the term), cranial settling, a kyphotic clivo-axial angle, and a retroflexed odontoid[12]. The kyphotic clivo-axial angle is an important and relatively easy measurement to indicate potential deformative stress on the brain stem. The clivus is a wedge-shaped bone that normally lies above and ventral to the top of spine. When it lies more horizontally, it creates a sharp angle that results in a bending of the brainstem. The odontoid peg (also called the odontoid process or the dens) is the part of the C2 vertebrae, or Axis, that the skull pivots upon, so named because of its tooth-like shape. A retroflexed odontoid occurs when the odontoid is bent backwards, often compressing the front of the brain stem. Other important measurements involving ventral brain stem compression for a kyphotic clivo-axial angle and/or retroflexed odontoid include the Grabb-Oakes and Harris measurements.
- The clivoaxial angle is measured by drawing a line along the posterior (back, or when lying more horizontal, the top) side of the lower clivus and intersecting that line with a line drawn on the posterior side of the axis. If the angle created is less than 135°, it is considered pathological. Like instability, a kyphotic clivoaxial angle is often seen in patients with connective tissue disorders and degenerative rheumatoid disease[13]. See figure 1 below.
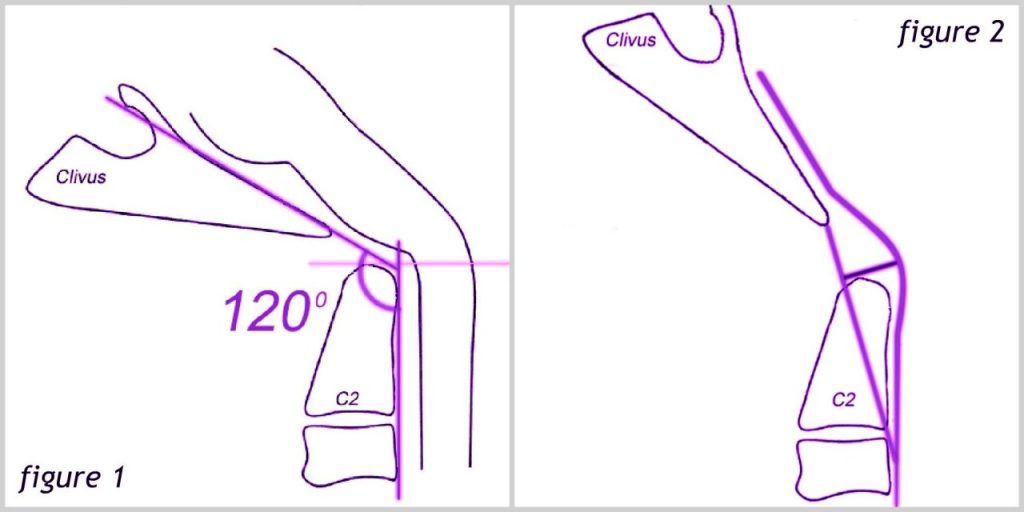
For the Grabb-Oakes measurement, a line is drawn from the basion (the midpoint of the anterior margin of the foramen magnum) to the inferior posterior C2. A perpendicular line is then drawn from the center of this line to the dura of the brain stem. A Grabb-Oakes measurement greater than 9 mm denotes a form of basilar invagination. This is a very helpful measurement for determining how much a retroflexed odontoid is compressing the brain stem. See Figure 2 above.
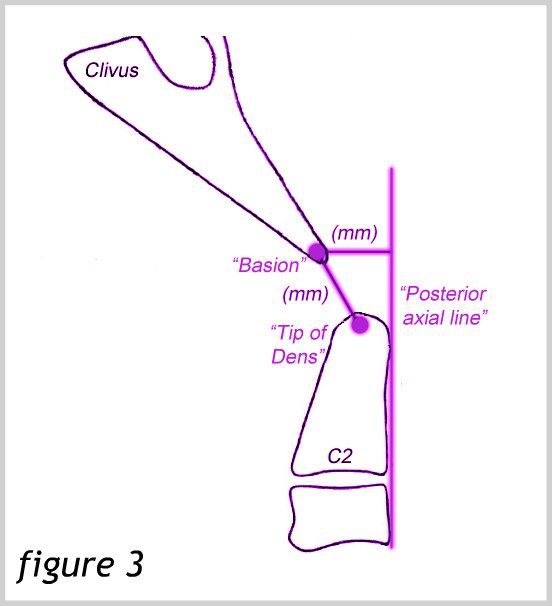
The Harris measurement is the distance between the basion and the Posterior Axial Line. This distance should not be more than 12 mm. A measurement of more than 12 mm also denotes instability. This measurement can also be used to measure the translation between flexion and extension in dynamic imaging[14]. See Figure 3.
Symptoms of ventral brain stem compression can occur with various types of BI and instability. They may be referred to together as a “cervicomedullary syndrome” and may include[15]:
- A heavy headache (often referred to as feeling like a “bobblehead” or feeling like the head is a “bowling ball”)
- A Chiari-type pressure headache aggravated by Valsalva maneuvers (because these conditions, like Chiari, can also cause flow issues)
- Dysautonomia (including tachycardia, heat intolerance, orthostatic intolerance, syncope (fainting), polydipsia (extreme thirst), delayed gastric emptying, chronic fatigue)
- Neck pain (often severe)
- Central or mixed sleep apnea
- Facial pain or numbness – Occasionally, including Trigeminal Neuralgia
- Balance and coordination impairment
- Muscle weakness
- Dizziness and vertigo
- Vision problems, including double vision and downward nystagmus
- Reduced gag reflex and dysphagia (difficulty swallowing)
- Tinnitus (ringing in the ears) and hearing loss
- Nausea and vomiting
- Paralysis
- In more severe cases, non-epiform seizures have also been documented
In addition to producing significant pain and neurological symptoms, the compression and kinking of the brain stem can cause significant injury to the brain stem neurons by stretching the axons of the nerves to the point that they break and recoil, producing what are called “axon retraction bulbs” that can be seen on microscopic examination of the cells. The stress placed on the brain stem by both compressing and stretching simultaneously is much greater than the mere sum of these two mechanisms. Interestingly, during the flexion of the normal spine, it stretches 17% of its length. Research has shown that the axon of a giant squid fails when stretched to 20% if its length. Therefore, the normal motion of the human neck brings us very close to injuring our brain stem. Consequently, it only takes a slight alteration of our normal anatomy to cause injury to these delicate nervous tissues[16].
Treatment of Craniocervical Instability typically begins with more conservative medical management, such as neck bracing, activity limitation, physical therapy (including isometrics, sagittal balance, core strengthening and cardio), and pain management. Other causes of symptoms such as co-morbid conditions, multiple sclerosis, dystrophy, mitochondrial disorders, vitamin deficiencies and Lyme disease should be ruled out or treated. However, surgical intervention via a craniocervical fusion is indicated when the following criteria are met:
Severe headache or neck pain >7/10
AND cervicomedullary syndrome
AND neurological deficits referable to the craniocervical junction
AND radiological findings indicative of instability
Surgeons and patients alike should consider surgery after medical management has been maximized and the patient has shown a positive response to neck bracing[10].
Various specific surgical techniques are applied in craniocervical fusions. A more common technique is the open reduction and fusion stabilization procedure. This procedure involves stabilizing the head with screws, making an incision that exposes the occiput through C2, and fixing plates to the occiput which attach to the C1 and C2 (and sometimes C3) vertebrae with rods. A newer technique adapted by Dr. Paolo Bolognese is using a less invasive Chiari decompression surgery known as MIST (minimally invasive subpial tonsillectomy) along with a fusion using screws placed in the occipital condyles. Although the dura is opened to partially resect the tonsils, a duraplasty is not done. Advantages of this procedure include a smaller incision, smaller hardware, less bone removal, and a thicker bone for which to insert screws in the occiput. Risks of both methods include vertebral artery injury, and a slightly increased risk for segmental instability below the fusion, along with the standard risks of any surgical procedure, such as bleeding, infection, and complications from anesthesia. Both procedures demand the hands of a very skilled and experienced surgeon because vital structures lie in and around the area. Using condylar screws may increase the risk of injury to major vessels, particularly in the hands of a less experienced surgeon. An important cranial nerve also lies just deep to the occipital condyles, making precise screw placement extremely important. This may limit the procedure in becoming more widely used, but the resulting fusion may be stronger, despite the reduced amount of hardware[17].
In the presence of a retroflexed odontoid, an open reduction, fusion and stabilization procedure may be enough to relieve ventral brain stem compression. However, in more severe cases, a further surgery called an odontoidectomy may be needed to remove the odontoid process. This surgery may be done through the mouth or the nose[18].
Every Chiari patient should be aware of hereditary connective tissue disorders and the signs and symptoms of Craniocervical Instability and Basilar Invagination. Many neurosurgeons do not evaluate their patients for these conditions prior to performing Chiari decompression surgery, often resulting in the need for revision surgeries and poor results. Being an educated patient can help you ask the right questions and insist on the proper evaluation and testing to avoid the pitfalls that many other patients have faced.
References:
1 Bolognese, Paolo A, director. Surgical Techniques for Chiari Malformations. YouTube, American Syringomyelia Chiari Alliance Project, 16 Mar. 2015, <www.youtu.be/KfYmJnB6sPQ>.
2 Bolognese, Paolo A. “Modern Classification and Subclassification of Chiari Malformations.”YouTube, American Syringomyelia Chiari Alliance Project, 16 Mar. 2015, <www.youtu.be/ZQ9ZmquN-M0>.
3 Bolognese, Paolo A. “2016 ASAP CM/SM Conference – ‘Complex Posterior Fossa’ – Bolognese.” YouTube, American Syringomyelia Chiari Alliance Project, 7 Dec. 2016, <www.youtu.be/3jKH_DHadO8>.
4 Augustus A. White III, Manohar M. Panjabi, et al. “Clinical Biomechanics of the Spine.” By Augustus A. White III, <www.leomed.at/listhoscan/white_90.pdf>
5 The Pain Relief Foundation, The Pain Relief Foundation, <www.thepainrelieffoundation.com/craniocervical-instability/>.
6 Bolognese, Paolo. Complex Posterior Fossa revisions. YouTube. December 7, 2016. <www.youtu.be/3jKH_DHadO8>.
7 Menezes, Arnold H. “Craniovertebral Junction Anomalies: Diagnosis and Management.”Seminars in Pediatric Neurology, vol. 4, no. 3, Sept. 1997, <www.sempedneurjnl.com/article/S1071-9091(97)80038-1/fulltext>.
8 Yang, Sun Y., et al. “A Review of the Diagnosis and Treatment of Atlantoaxial Dislocations.”Global Spine Journal, Georg Thieme Verlag KG, Aug. 2014, <www.ncbi.nlm.nih.gov/pmc/articles/PMC4111952/>.
9 Henderson, Fraser C., et al. “Neurological and Spinal Manifestations of the Ehlers–Danlos Syndromes.” American Journal of Medical Genetics Part C: Seminars in Medical Genetics, <www.onlinelibrary.wiley.com/doi/10.1002/ajmg.c.31549/full>.
10 Henderson, Sr. , Fraser C. “Neurological Management of Hereditary Disoders of Hypermobility Connective Tissue Disorders.” Ehlers-Danlos Society Annual Conference 2015. Ehlers-Danlos Society Annual Conference 2015, 14 Aug. 2015, Baltimore, <www.ehlers-danlos.com/2015-annual-conference-files/Henderson_0.pdf>.
11 Hain, Timothy C. “Basilar Invagination, Basilar Impression and Atlantoaxial Subluxation.”Basilar Invagination, Basilar Impression and Atlantoaxial Subluxation, 19 Apr. 2013, <https://dizziness-and-balance.com/disorders/central/cerebellar/basilar_invagination.htm>.
12 Kim, Louis J., et al. “JNS JOURNAL OF Neurosurgery OFFICIAL JOURNALS OF THE AANS since 1944.” Treatment of Basilar Invagination Associated with Chiari I Malformations in the Pediatric Population: Cervical Reduction and Posterior Occipitocervical Fusion | Journal of Neurosurgery: Pediatrics, Vol 101, No 2, Nov. 2004, <www.thejns.org/doi/abs/10.3171/ped.2004.101.2.0189?url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org&rfr_dat=cr_pub%3Dpubmed>.
13 Henderson, Sr. , Fraser C. “Cranio-Cervical Instability in Patients with Hypermobility Connective Disorders.” OMICS International, OMICS International, 18 Apr. 2016, <www.omicsgroup.org/journals/craniocervical-instability-in-patients-with-hypermobility-connective-disorders-2165-7939-1000299.php?aid=71754#11>.
14 Bono, C M, et al. “Measurement Techniques for Upper Cervical Spine Injuries: Consensus Statement of the Spine Trauma Study Group.” Spine., U.S. National Library of Medicine, 1 Mar. 2007, <www.ncbi.nlm.nih.gov/pubmed/17334296>.
15 Henderson, Sr. , Fraser C. “Diagnosis and Treatment of Craniocervical Instability in the Chiari Patient.” Chiari and Syringomyelia Foundation Educational Lecture. 20 July 2011, Greater Metropolitan Washington Area, Greater Metropolitan Washington Area, <www.youtu.be/U33T8JFXvk0>.
16 Henderson, F C, et al. “Neuropathology of the Brainstem and Spinal Cord in End Stage Rheumatoid Arthritis: Implications for Treatment.” Annals of the Rheumatic Diseases, U.S. National Library of Medicine, Sept. 1993, <www.ncbi.nlm.nih.gov/pmc/articles/PMC1005138/>.
17 Bolognese, Paolo A. “Surgical Techniques for Chiari Malformations.” YouTube, American Syringomyelia Chiari Alliance Project, 16 Mar. 2015, <www.youtube.com/watch?v=KfYmJnB6sPQ>.
18 Hwang, Steven W., et al. “C1–C2 Arthrodesis after Transoral Odontoidectomy and Suboccipital Craniectomy for Ventral Brain Stem Compression in Chiari I Patients.”European Spine Journal, Springer-Verlag, Sept. 2008, <www.ncbi.nlm.nih.gov/pmc/articles/PMC2527411/>.